




What Is a Certificate of Medical Necessity?
A certificate of medical necessity (CMN) is a document that establishes, in clinical terms, why a specific patient requires a specific piece of durable medical equipment. In the US, it was originally a standardized form required by CMS to substantiate in detail the medical necessity of an item of durable medical equipment or a service to a Medicare beneficiary.
Historically, the CMN served a dual purpose: it captured the physician’s clinical justification for the equipment, and it also functioned as the written order for certain product categories. For items that required a CMN, and for accessories, supplies, and drugs related to an item requiring a CMN, the CMN could serve as the written order if the narrative description in Section C was sufficiently detailed.
The form had four sections, A through D. Suppliers could complete sections A and C — patient information and equipment details. Sections B and D required the ordering physician’s signature and clinical attestation. A claim submitted without a complete, signed CMN for a covered item was a claim at risk of denial.
What Happened to the CMN Form?
Effective January 1, 2023, CMS no longer requires Certificates of Medical Necessity and DME Information Forms for selected durable medical equipment. This documentation was originally required to help confirm medical necessity and other coverage criteria. Historically, DME suppliers would receive a signed certificate from the treating physician or a signed form to submit with each claim. However, information from these documents is now available either on the claim or in the medical record.
The elimination of the physical CMN form was part of a broader CMS push to reduce administrative burden on suppliers and physicians. But the policy change created a significant source of confusion in the industry, and that confusion has direct billing consequences.
Removing the form did not remove the requirement to document medical necessity. It shifted where that documentation must live. The Standard Written Order (SWO) replaced older forms such as Certificates of Medical Necessity and Delivery/Installation Forms, though a complete SWO must still be supported by the patient’s clinical records to avoid claim denials.
This means that when a billing manager or intake coordinator today refers to “getting the CMN,” they’re typically talking about one of three things: collecting the Standard Written Order from the prescribing physician, gathering supporting clinical records that establish medical necessity, or (for product categories still requiring it), obtaining prior authorization before delivery.
What Is CMN in Medical Billing Today?
In practical DME billing usage in 2026, “CMN” functions as umbrella shorthand for the documentation package that proves a patient qualifies for covered equipment. That package has specific components, each of which must be in place before a clean claim can go out the door.
Standard Written Order (SWO)
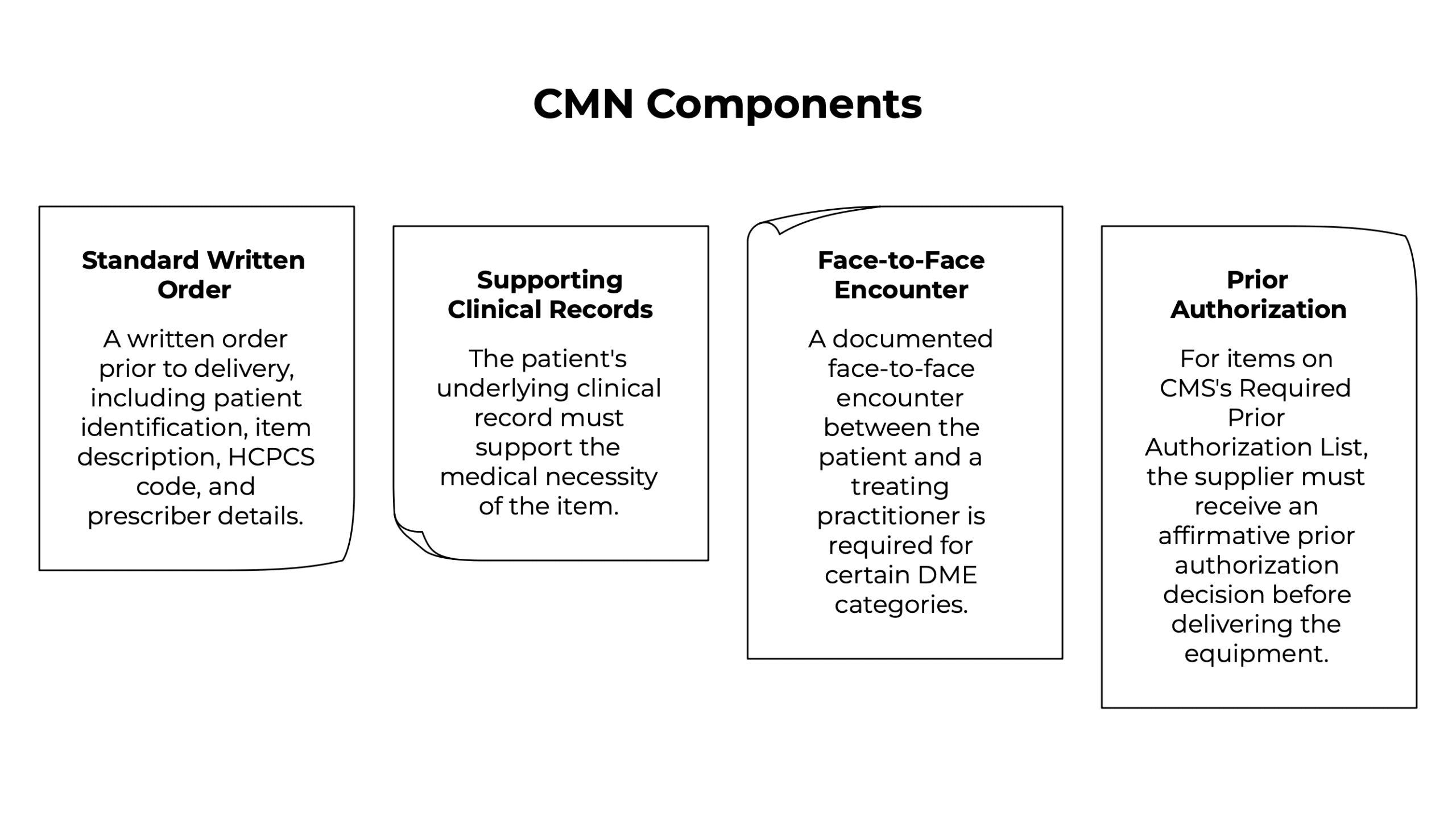
Before submitting a claim to Medicare, the DMEPOS supplier must have on file an SWO, a written order prior to delivery (if applicable), information from the treating practitioner concerning the patient’s diagnosis, and any information required for the use of specific modifiers or attestation statements as defined in certain DME MAC policies. The SWO must include patient identification, item description, HCPCS code, and prescriber details, all signed and dated.
Supporting clinical records
The SWO alone is not sufficient. Medicare requires that the patient’s underlying clinical record supports the medical necessity of the item. The Medicare Appeals Council concluded that a supplier had claimed Medicare payment with only a CMN as support, so the equipment was not covered by Medicare — a precedent that established the principle that medical necessity must be documented in the record, not just attested to on a form.
Face-to-face encounter documentation
For certain high-value DME categories (particularly power mobility devices) a documented face-to-face encounter between the patient and a treating practitioner is required before the written order can be completed. The encounter must be documented in the clinical record, and the written order must be completed within six months of that encounter.
Prior authorization
For items on CMS’s Required Prior Authorization List, the supplier must receive an affirmative prior authorization decision before delivering the equipment. Delivering first and billing later on these items is not an option — the claim will be denied.
CMN for Durable Medical Equipment: Which Items Still Require What
The shift away from the formal CMN form means documentation requirements now vary by product category, and staying current with what each category requires is a direct billing competency.
Medicare requires a Standard Written Order for each DME item being billed. Beyond that baseline, certain categories carry additional requirements:
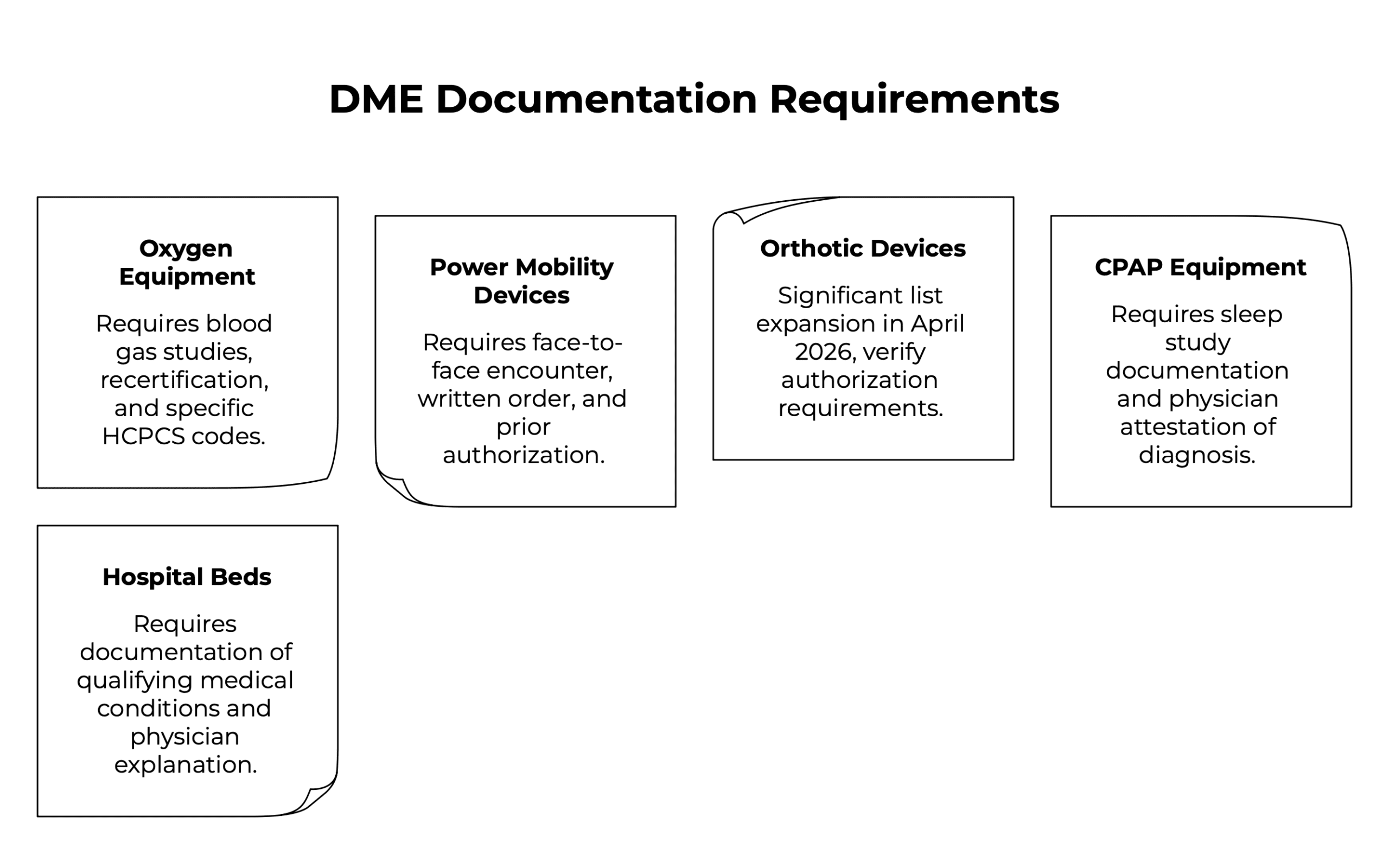
- Oxygen equipment remains one of the most documentation-intensive DME categories. Qualifying blood gas studies must be on file and must meet specific thresholds. Recertification documentation is required at defined intervals. Eight oxygen-related HCPCS codes were added to CMS’s Face-to-Face and Written Order Prior to Delivery list in the January 2026 Federal Register update.
- Power mobility devices (power wheelchairs and scooters) require a face-to-face encounter, a written order prior to delivery, and prior authorization in most jurisdictions. These have been on the Required Prior Authorization List for years precisely because they were historically high-risk for improper billing.
- Orthotic devices saw significant list expansion in April 2026. Seven new codes were added to the Required Prior Authorization List effective April 13, 2026, with most of these codes being for orthotic devices. Suppliers billing L-codes for lumbar, knee, and ankle-foot orthoses need to verify authorization requirements against the current list before delivery.
- CPAP and respiratory therapy equipment requires sleep study documentation and physician attestation of diagnosis. The clinical records supporting medical necessity (polysomnography results, AHI scores, physician notes) must be on file and must match the diagnosis codes billed.
- Hospital beds and pressure-relief mattresses require documentation of qualifying medical conditions and, in many cases, a physician’s narrative explanation of why standard alternatives are insufficient.
The operational implication: your intake team needs product-category-specific documentation checklists, not a single generic “CMN checklist” applied across all order types. An oxygen order and a power wheelchair order have almost nothing in common in terms of documentation requirements.
How Documentation Gaps Drive Claim Denials
Missing or incomplete Certificate of Medical Necessity documentation is one of the most common root causes of DME billing errors and subsequent denials. The downstream cost is real: a denied claim doesn’t just delay payment. It triggers a rework cycle that consumes billing staff time, risks timely filing deadlines if not caught quickly, and becomes a write-off if it falls through the cracks entirely.
The most common documentation failures in DME medical necessity billing fall into a predictable pattern. Missing physician signature on the written order — often because the order was sent to a practice and never followed up on. Clinical records that don’t explicitly support the diagnosed condition. Equipment delivered before prior authorization was confirmed for a code on the Required Prior Authorization List. Recertification documentation not collected when a rental patient hits a renewal period.
If the information in the patient’s medical record does not adequately support the medical necessity for the item, the supplier is liable for the dollar amount involved unless a properly executed Advance Beneficiary Notice of Noncoverage has been obtained. That liability exposure is not theoretical — Medicare audits actively target documentation gaps in high-risk DME categories.
The fix is upstream. Catching documentation problems at intake (before the equipment leaves the warehouse) costs a fraction of what it costs to work a denied claim or respond to a post-payment audit.
Prior Authorization and CMN: How They Connect
Prior authorization and medical necessity documentation are not the same process, but they are tightly linked. Prior authorization is the mechanism by which Medicare or another payer reviews the documentation and confirms coverage eligibility before delivery. Medical necessity documentation is the substance of what gets reviewed.
Under the CMS Interoperability and Prior Authorization Final Rule that went into effect January 1, 2026, standard prior authorization decisions now have a 7 calendar day limit, and denials now require a specific reason. For DME suppliers, the shorter decision window is operationally useful (it means you can expect a faster turnaround on auth requests), but it also means your documentation needs to be complete when you submit, not assembled reactively after a denial.
Practices billing for DME should check the CMS DMEPOS prior authorization list regularly, as it is updated periodically. The April 2026 expansion added orthoses and pneumatic compression devices. Earlier cycles added power mobility codes. The list will continue to grow as CMS tightens oversight of high-cost categories.
The practical workflow: before any order is accepted for a code that might be on the Required Prior Authorization List, the billing or intake team should verify against the current list, confirm documentation requirements for that code, and initiate the prior authorization request before scheduling delivery.
Managing CMN Documentation With Software
Manual CMN and medical necessity documentation workflows, tracking outstanding physician orders in a spreadsheet, following up on missing signatures via phone, storing clinical records in a filing system disconnected from your billing platform, create the exact conditions that produce documentation gaps and denials.
A capable DME billing platform needs to track CMN expiration dates, store physician-signed documentation, and flag orders where documentation is incomplete or out of date.
NikoHealth’s patient intake and order management workflows are built around this requirement. When an order comes in, the system tracks documentation status in real time (outstanding physician signatures, missing clinical records, prior authorization requests and responses), so your billing team knows what’s complete and what’s at risk before a claim is ever submitted. Automated eligibility verification runs at intake, and pre-submission compliance checks flag documentation gaps before equipment leaves the warehouse.
The result is fewer denials from preventable documentation failures, shorter AR cycles, and a billing team that spends its time on exceptions rather than chasing paperwork that should have been complete at order entry.

FAQ
What is a CMN in medical billing?
In DME medical billing, CMN stands for Certificate of Medical Necessity. CMS discontinued the formal CMN form for most equipment categories effective January 1, 2023. Today, “CMN” broadly refers to the documentation package that establishes a patient’s medical need for durable medical equipment, including the Standard Written Order, supporting clinical records, and prior authorization where required.
What is a certificate of medical necessity form for DME?
The certificate of medical necessity was a standardized, four-section form that Medicare required DME suppliers to collect from the ordering physician before submitting claims for certain equipment categories. CMS eliminated the physical form in January 2023. The underlying documentation requirements — physician order, clinical justification, and supporting medical records — remain mandatory and must now be captured in the patient’s record.
Does CMN still exist for durable medical equipment?
The formal CMN form no longer exists for most DME categories billed to Medicare for dates of service on or after January 1, 2023. However, the documentation requirements the form captured (medical necessity justification, physician attestation, and clinical records) are still required and must be on file before a claim is submitted. Some commercial payers and state Medicaid programs may still use CMN-style forms.
What is the difference between CMN and prior authorization for DME?
A CMN (or equivalent medical necessity documentation) establishes why a patient needs specific equipment. Prior authorization is a pre-delivery review process in which a payer confirms coverage eligibility based on that documentation. For items on CMS’s Required Prior Authorization List, a supplier must receive prior authorization approval (not just have documentation on file) before delivering equipment to a Medicare beneficiary.
What documentation replaces the CMN for Medicare DME billing?
The Standard Written Order (SWO) is the primary document replacing the CMN for Medicare DME billing. The SWO must include patient identification, item description, and prescriber information. For most equipment categories, the SWO must be supported by clinical records documenting the patient’s diagnosis and medical need. For higher-value or high-risk equipment, face-to-face encounter documentation and prior authorization are also required.

With over a decade of experience in medical software and hardware support, Alan combines technical expertise with hands-on client collaboration to help organizations achieve successful implementations.

Related Articles