




Claim denials are one of the biggest revenue drains in the DME industry. A rejected claim doesn’t just delay payment – it creates rework, eats up your billing team’s time, and, if it falls through the cracks, can mean you never collect at all. The good news? Most DME claim errors are preventable.
This guide breaks down what DME claims are, how DME claims processing works, and the best practices that help providers collect faster and deny less.
What Are DME Claims?
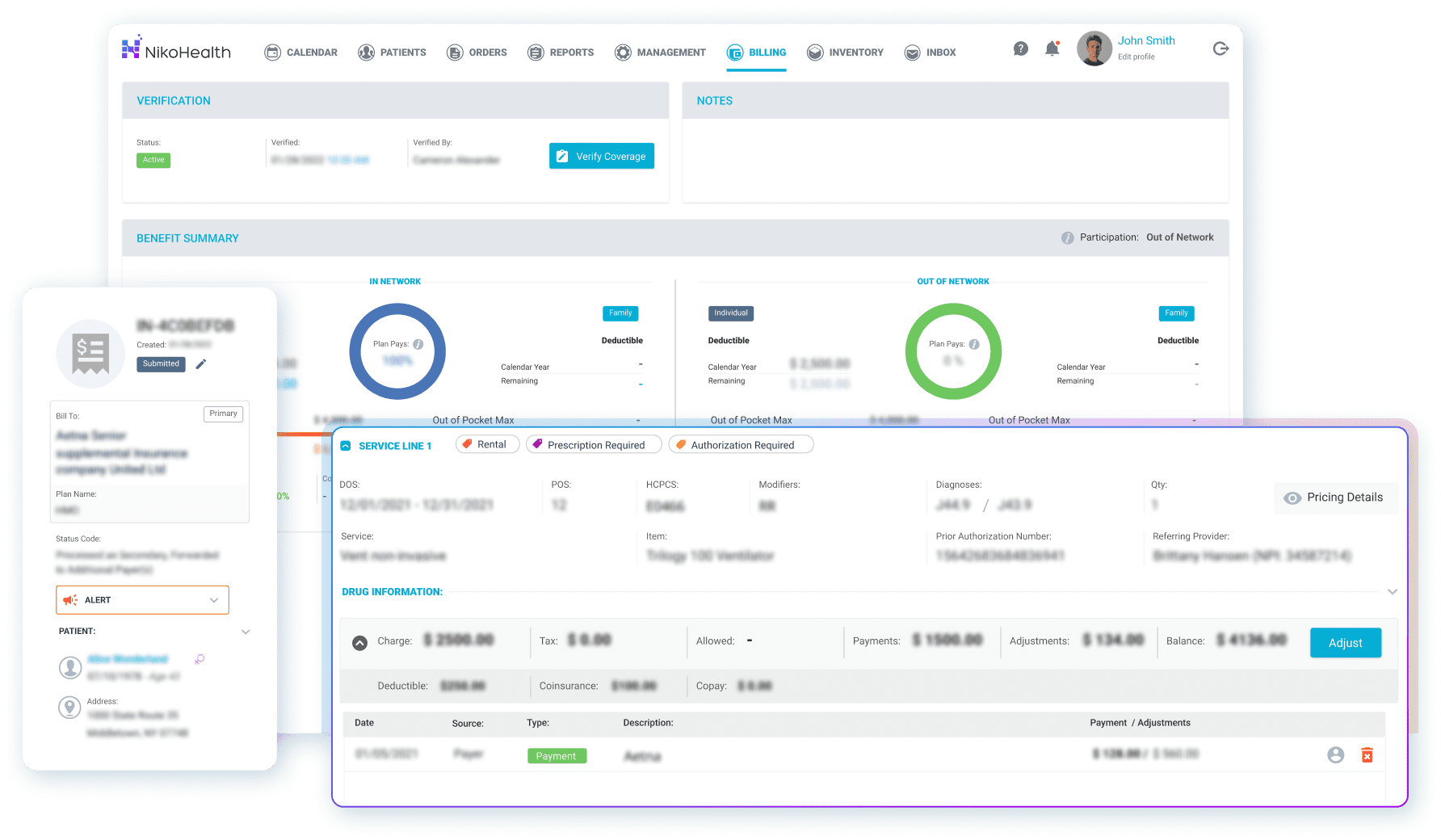
DME claims are formal reimbursement requests submitted by HME/DME providers to payers (Medicare, Medicaid, or private insurers) to receive payment for durable medical equipment supplied to a patient.
The DME claims meaning goes beyond a simple invoice. Each claim is a structured data submission that must include the correct HCPCS codes, patient and prescriber details, a valid Certificate of Medical Necessity (CMN) where required, and documentation that the equipment was actually delivered and meets the payer’s coverage criteria.
💡In short: a DME claim is both a billing document and a compliance document. Get either part wrong, and you’re looking at a denial.
How Does DME Claims Processing Work?
DME claims processing is the end-to-end workflow that takes a patient order from intake through to final payment. For most providers, that journey looks something like this:
- Insurance eligibility verification. Before anything ships, your billing team confirms the patient’s coverage, deductibles, and any prior authorisation requirements.
- CMN and documentation. A Certificate of Medical Necessity is obtained from the prescribing clinician, along with any clinical notes the payer requires.
- Order processing and delivery. Equipment is picked, dispatched, and delivered. Delivery confirmation (including patient signature) is captured.
- Claim creation and scrubbing. The claim is built with the correct HCPCS codes, modifiers, and billing information, then checked for errors before submission.
- Claim submission. Claims are submitted electronically via an approved clearinghouse.
- Payment posting. When payment arrives, remittances (ERA/EOB) are posted against the claim. Underpayments and denials are flagged for follow-up.
- Denial management. Rejected claims are reviewed, corrected, and resubmitted within payer timely filing windows.
Each of these steps is a potential failure point. Manual processes at any stage increase the risk of errors that translate directly into delayed or lost revenue.

DME Claims Best Practices
1. Verify Eligibility at Every Intake – Not Just Once
Payer coverage changes. A patient who was fully covered three months ago may have switched plans, hit their deductible, or lost coverage entirely. Run eligibility verification at the point of every new order, not just at initial patient setup.
Catching a coverage issue before equipment ships is a five-minute fix. Chasing a denied claim after the fact can take weeks.
2. Get Your CMN Documentation Right the First Time
Missing or incomplete CMN documentation is one of the most common reasons DME claims get denied by Medicare and private payers. Make sure your intake process captures all required clinical information upfront – diagnosis codes, prescriber NPI, and clinical justification that matches the equipment being ordered.
If your team is chasing down CMN corrections after delivery, that’s a process problem, not a one-off issue.
3. Use Claims Scrubbing Before Every Submission
Claims scrubbing, running each claim through automated validation checks before it reaches the payer, catches billing errors that would otherwise result in denials. Common issues it catches include mismatched diagnosis and HCPCS codes, missing modifiers, duplicate claim submissions, and incorrect units or date ranges for recurring rentals.
Providers who scrub claims before submission consistently see lower first-pass denial rates. It’s one of the highest-leverage steps in billing DME claims.
4. Don’t Let Recurring Rental Claims Fall Through the Gaps
Recurring rentals are one of the most profitable (and most error-prone) parts of DME billing. Monthly invoicing cycles, ongoing CMN renewals, and capped rental rules all create complexity that’s easy to miss when you’re managing billing manually.
Automating your recurring rental invoicing means every cycle generates correctly, with the right billing codes for the rental month, rather than relying on someone to remember to run it.
5. Track Denial Reasons Systematically
Not all denials are equal. Some are administrative (wrong NPI, missing field) and easy to fix. Others signal a deeper problem – a payer rule change, a documentation gap in your workflow, or a recurring billing code error.
If you’re only fixing individual denials without tracking why they happened, you’ll keep fixing the same ones. Grouping denials by reason code and payer gives you the data to fix root causes, which is where the real revenue recovery happens.
6. Know Your Timely Filing Windows
Every payer has a timely filing deadline — the window within which a claim must be submitted after the date of service. Miss it, and the claim is denied with essentially no appeal path.
For Medicare, the standard window is 12 months. Private payers can be as short as 90 days. If your denial management workflow doesn’t flag claims approaching their filing deadline, you’re at risk of writing off revenue that should have been collectable.
7. Post Remittances Promptly, and Reconcile Everything
Manual ERA/EOB processing is slow, tedious, and prone to posting errors. When remittances sit unprocessed, you lose visibility into your actual collections position and miss underpayments that need follow-up.
Automated remittance posting clears the backlog and gives your billing team a clean accounts receivable picture – so they’re chasing the right outstanding claims, not trying to reconcile last month’s payments.
Common DME Claims Errors to Avoid
Errors that cause the most DME claim denials:
- Missing or expired CMN documentation
- Incorrect HCPCS codes or modifiers for the equipment supplied
- Prior authorisation not obtained before delivery
- Billing outside the payer’s coverage criteria for the diagnosis
- Duplicate claims submitted for the same date of service
- Wrong billing NPI or provider enrollment issues
- Timely filing windows missed on resubmissions
Most of these are preventable with the right workflow and automated checks in place.
How Technology Improves DME Claims Processing
Managing DME claims processing manually (across spreadsheets, fax queues, and legacy software) works until it doesn’t. As claim volume grows, so does the risk of errors slipping through. Modern billing DME software automates the steps most likely to cause problems.
NikoHealth, for example, handles eligibility verification, claims scrubbing, and remittance posting automatically, reducing the manual touchpoints where errors creep in. When a claim is denied, the denial management workflow surfaces it immediately, with the reason code, so your team can act rather than hunt.
Providers who move from manual or fragmented billing processes to an integrated platform consistently report measurable improvements: faster collection cycles, fewer denials, and billing teams that spend their time on exceptions rather than routine data entry.
Manual vs. Automated DME Claims Processing
| Manual Process | Automated with Modern Software |
| Eligibility checked manually per order | Eligibility verified automatically at intake |
| CMN tracking in spreadsheets or paper files | CMN status tracked within the order workflow |
| Claims scrubbed by reviewer before submission | Automated pre-submission compliance checks |
| ERA/EOB posted manually by billing staff | Remittances posted automatically |
| Denials tracked in a spreadsheet or ignored | Denial management queue with reason codes |
| Recurring rentals manually invoiced each cycle | Recurring billing generated automatically |
Frequently Asked Questions
What is the difference between a DME claim and a regular medical claim?
A DME claim specifically requests reimbursement for durable medical equipment — items like wheelchairs, oxygen concentrators, CPAP machines, and hospital beds. Unlike physician or facility claims, DME claims often require additional documentation such as a Certificate of Medical Necessity, prior authorisation, and delivery confirmation. They also frequently involve recurring rental billing, which adds complexity that standard medical claims don’t have.
Why do DME claims get denied more often than other claim types?
DME claims carry a higher documentation burden than most medical claims. Payers require proof that the equipment was medically necessary, that it was actually delivered, and that it meets specific coverage criteria. Any gap in that documentation chain (an expired CMN, a missing modifier, or a diagnosis code that doesn’t align with the equipment billed) is grounds for denial. Add in the complexity of recurring rentals, capped rental rules, and frequent payer policy changes, and it’s a category where errors are easy to make and expensive to miss.
How long does DME claims processing typically take?
With electronic submission, most payers process clean DME claims within 14 to 30 days. Medicare typically processes electronic claims in 14 days. Private payers vary – some process within two weeks, others can take 30 to 45 days. Denied claims that require correction and resubmission can add weeks or months to the collection cycle, which is why first-pass clean claim rates matter so much to revenue cycle management performance.
What is claims scrubbing in DME billing?
Claims scrubbing is the process of checking a claim for errors before it’s submitted to a payer. Automated scrubbing tools validate HCPCS codes, modifiers, diagnosis codes, provider information, and other required fields against payer rules. The goal is to catch and fix errors before the claim reaches the payer, rather than dealing with a denial after the fact. Providers who scrub claims before submission consistently achieve higher first-pass acceptance rates.
What happens when a DME claim is denied?
When a payer denies a DME claim, they issue an Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA) that includes a reason code explaining why. The billing team reviews the denial, corrects the issue (whether that’s updated documentation, a corrected billing code, or an appeal) and resubmits within the payer’s timely filing window. Claims not addressed within that window are typically written off, which is why a structured denial management workflow is essential.
Summary
DME claims processing is one of the most complex parts of running an HME/DME business, but most of the errors that cause denials and revenue loss are preventable. Strong eligibility verification at intake, accurate CMN documentation, claims scrubbing before submission, and systematic denial tracking are the foundations of a high-performing billing operation.
The providers that collect more consistently are the ones who’ve removed manual handoffs from the process and built a workflow where errors get caught before they reach the payer, not after.


Related Articles