




What Does a Medical Supply Business Actually Make?
Gross margins in the medical supply and DME industry are not retail margins. When you’re billing Medicare, Medicaid, or commercial payers, you don’t set prices — the payer’s fee schedule does. For most DMEPOS product categories, Medicare reimbursement rates are fixed, and in competitive bidding areas (CBAs), they’ve been compressed further over the past decade.
A realistic gross margin for a small-to-mid-size DME supplier falls between 23% and 35%, depending on product mix. Higher-margin categories include power wheelchairs, sleep therapy equipment (CPAP/BiPAP), and orthotics. Lower-margin categories include standard beds, ambulatory aids, and basic wound care supplies.
Net margin (after billing staff, delivery, DME compliance costs, and software) typically lands between 8% and 15% for well-run operations. Businesses running inefficient billing workflows or high denial rates frequently see net margins below 5%.
The profitability driver most operators underestimate: the cost of a denied claim. Every claim that gets rejected costs staff time to rework, delays payment by 30–60 days, and (if not caught) becomes a write-off. A business doing $2 million in annual billings with a 12% denial rate is leaving roughly $240,000 in revenue at risk every year.
How Much Does It Cost to Start a Medical Supply Business?
Startup costs vary significantly based on whether you’re opening a storefront, operating as a delivery-only supplier, or focusing exclusively on a niche product category like respiratory or orthotics. The ranges below reflect realistic costs for a small-to-mid-size HME/DME operation entering the market in 2026.
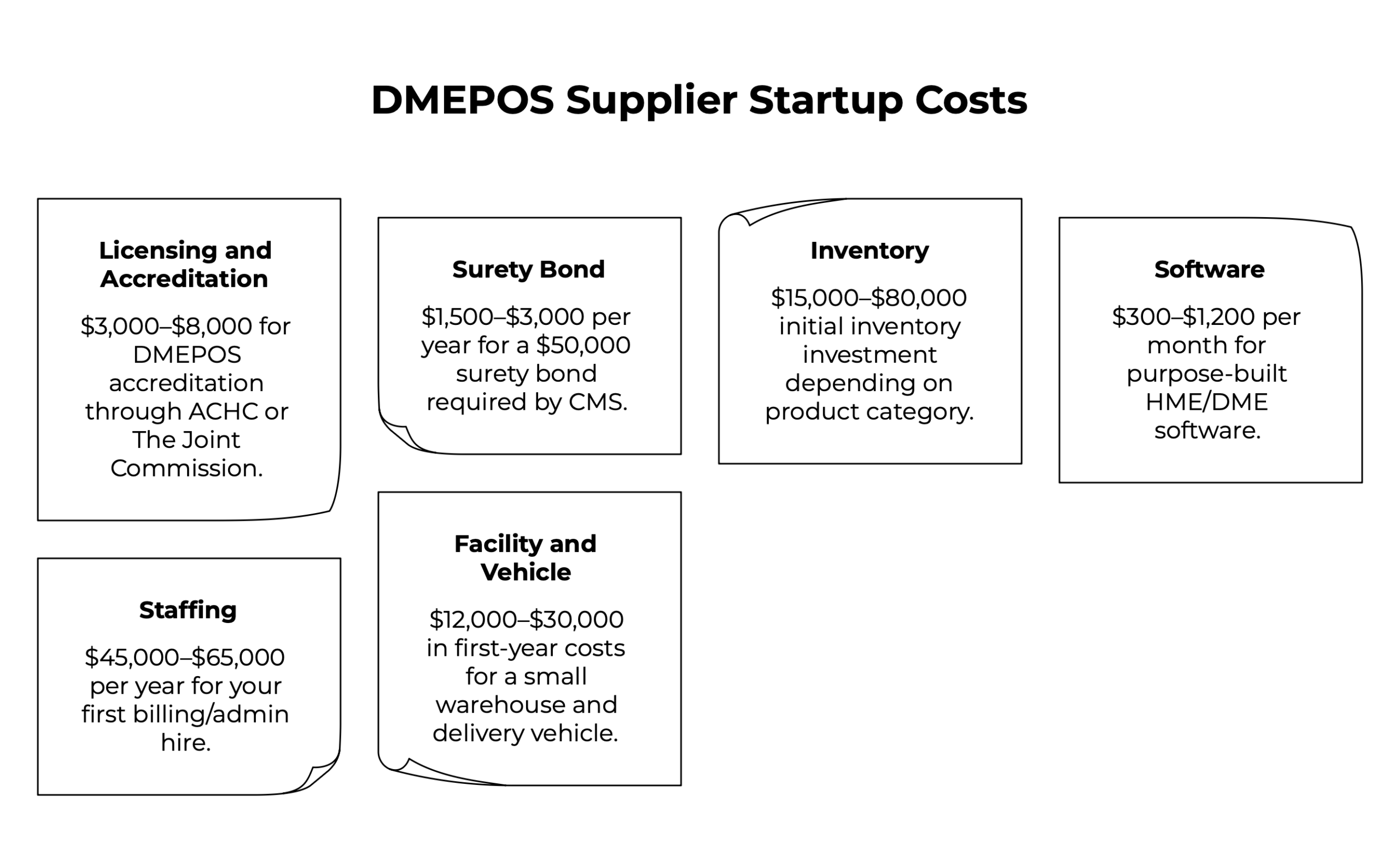
Licensing and accreditation
$3,000–$8,000 DMEPOS accreditation through ACHC or The Joint Commission is mandatory to bill Medicare and Medicaid. This includes the accreditation fee, facility inspection, and the preparation time to document your quality management processes. Factor in 3–6 months for the full process.
Surety bond
$1,500–$3,000 per year CMS requires a $50,000 surety bond for all DMEPOS suppliers. Annual premiums depend on your credit profile but typically run 2–4% of the bond amount.
Inventory
$15,000–$80,000 Initial inventory investment depends heavily on your product category. A respiratory-focused operation can launch with 20–30 CPAP units and related accessories. A full-service HME supplier needs beds, walkers, wheelchairs, and wound care inventory.
Software
$300–$1,200 per month Purpose-built HME/DME software covers billing, inventory, order management, and delivery. This is not an area to cut costs — manual billing in a payer-fee-schedule environment leads directly to claim errors, denials, and delayed collections.
Staffing
$45,000–$65,000 per year for your first billing/admin hire Your first employee is almost always a billing or intake coordinator. Getting DME claims right from day one is more important than any other operational investment.
Facility and vehicle
$12,000–$30,000 in first-year costs A small warehouse or retail location plus a delivery vehicle. Some operators start with a home-based warehouse setup to reduce early overhead, which is viable for delivery-only models.
💡 Total first-year costs for a lean, single-location operation: $80,000–$200,000, depending on inventory depth and staffing decisions.
The Medical Supply Business Plan: What Lenders and Investors Actually Want to See
If you’re writing a medical supply business plan to secure financing or bring on a partner, the financial section needs to reflect the realities of DME billing, not generic retail projections.
Lenders with experience in healthcare services will look for three things your plan must address directly.
- Payer mix and reimbursement rates. Document your target payer mix — what percentage of revenue will come from Medicare, Medicaid, and commercial insurance versus private pay. Show that you understand the reimbursement rates for your core product categories. Generic revenue projections without payer-specific assumptions will immediately signal inexperience.
- Claims cycle and cash flow timing. Medicare typically pays within 14–30 days of a clean claim submission. Build your cash flow model around realistic collection timelines. If you’re projecting cash flow based on delivery dates rather than payment receipt dates, your runway estimates will be wrong.
- Compliance infrastructure. Detail your accreditation status, documentation workflows, and how you’ll manage prior authorization requirements. For capped rental categories like power wheelchairs, show that your billing processes handle the rental-to-purchase conversion correctly — this is a common compliance failure for new suppliers.
A strong medical supply business plan also defines your geographic service area and referral strategy. DME businesses live and die by referral relationships — with physicians, discharge planners, home health agencies, and hospice providers. Lenders want to see that you have a realistic plan to build those relationships, not just a list of product categories.
What Makes the Difference Between Profitable and Struggling?
The operational gap between DME businesses that hit 12–15% net margins and those stuck below 5% comes down to a small number of controllable factors.
Denial rate management
The national average claim denial rate for DME suppliers is around 15–20%. High-performing operations run below 5%. The difference is almost entirely upstream: clean intake, eligibility verification before delivery, and automated pre-submission scrubbing. Every percentage point of denial reduction goes directly to the bottom line.
Accounts receivable discipline
Slow collections are a profitability killer in this industry. DME businesses that let AR age past 90 days on Medicare claims are often dealing with documentation gaps that could have been resolved at intake. Practices that run automated remittance posting and systematic follow-up on outstanding claims consistently collect more of what they bill.
Inventory management
Overstocked inventory ties up capital. Understocked inventory delays fulfillment and strains referral relationships. Real-time inventory visibility, knowing what’s on the shelf, what’s on loan to patients, and what needs to be serviced, directly affects both cost control and revenue.
Software infrastructure
Running billing in one system, inventory in another, and delivery tracking in spreadsheets is the single most common reason DME businesses plateau. The data gaps between disconnected systems create billing errors, lost rental cycles, and compliance exposure. Operators who bring everything into one platform (billing, inventory, order management, delivery) report material improvements in collections speed and staff efficiency.
NikoHealth is built for exactly this environment. It consolidates billing automation, inventory, order management, and delivery into a single cloud-based platform designed specifically for HME/DME providers, so your team spends less time correcting errors and more time collecting revenue.
Is It Still Worth Starting a Medical Supply Business in 2026?
The fundamentals are genuinely favorable. The US population over 65 is growing faster than at any point in modern history. Home-based care is becoming the default model for post-acute and chronic disease management. Demand for DME and HME services is structural, not cyclical.
But the window for underprepared entry is closing. CMS audits, competitive bidding pressures, and state-level surety requirements have raised the bar for new suppliers. Businesses that launch without accreditation, without solid billing infrastructure, or without a clear referral strategy spend their first 18 months fixing compliance problems instead of building volume.
The operators who enter this market successfully in 2026 share common traits: they understand the payer environment before they open, they invest in billing infrastructure early, and they treat referral relationship development as a core business function from day one.
Profitable medical supply businesses are not built on margins alone — they’re built on operational discipline in a billing-intensive, compliance-heavy environment. Get the foundation right, and the demand is there to support a durable, growing business.
FAQ
Is a medical supply business profitable?
Yes, medical supply businesses can be profitable, with net margins typically ranging from 8% to 15% for well-run operations. Profitability depends on denial rate management, collections speed, and operational efficiency, not just product volume or payer reimbursement rates.
How much does it cost to start a medical supply business?
Starting a small-to-mid-size HME/DME operation typically requires $80,000–$200,000 in first-year capital, covering DMEPOS accreditation, surety bond, initial inventory, software, and staffing. Costs vary based on product category and whether you operate a storefront or delivery-only model.
What licenses do you need to start a medical supply company?
You need DMEPOS supplier accreditation from an approved accreditation organization (such as ACHC or The Joint Commission), a CMS-required $50,000 surety bond, a state DME supplier license, and a National Provider Identifier (NPI). These are prerequisites for billing Medicare and Medicaid.
What should a medical supply business plan include?
A medical supply business plan should cover your payer mix and reimbursement rate assumptions, cash flow projections based on realistic claims collection timelines, your compliance and accreditation infrastructure, and a referral development strategy. Generic revenue projections without payer-specific details will not hold up to lender scrutiny.
How long does it take to become profitable in the medical supply business?
Most small DME suppliers reach operational breakeven within 12–18 months, provided they achieve DMEPOS accreditation on schedule, build referral volume steadily, and maintain clean billing workflows from the start. Operations with high denial rates or poor AR discipline can take significantly longer to reach positive cash flow.


Related Articles